Home
Why Choose Us
Our Quality
Testimonials
The Team
Dentists
Support Staff
Treatments
Fees
CPD Events
Referrals
Referral Form
Criteria for Referrals
Patient Feedback
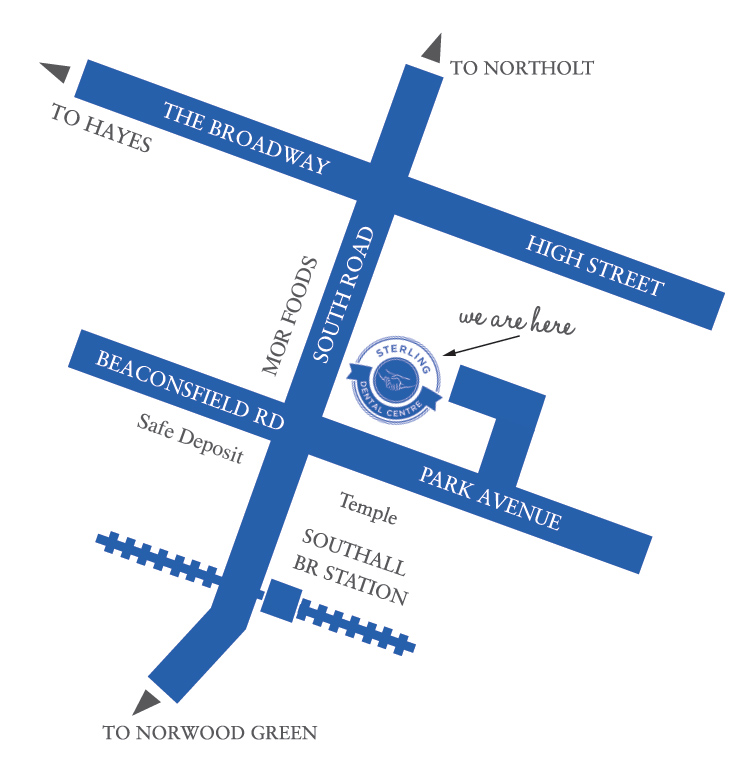
Contact Us
Referral Form
Referral Form (Sterling Dental Centre)
Surgery Details
Surgery Name & Address
*
Phone Number
*
Surgery Email
*
Clinicians Name
*
Total charge for NHS
*
Paid here
Pay later
Patient Details
Surname
*
Forename
*
Title
*
Mr
Mrs
Miss
Ms
Dr
Sex
*
M
F
Date of Birth
*
Address
*
City
*
Country
Postcode
*
Patient Mobile No.
*
Patient Email
*
Referral service to provider for:
– IV
– RA
– LA
Treatment to be provided (Including Medical History & any other information):
Upload the attachment (X-Ray Mandatory):
Drop a file here or click to upload
Choose File
Maximum file size: 104.86MB
Submit and download PDF
If you are human, leave this field blank.
NHS Services
Oral surgery under local
Oral surgery under Sedation
General Dentistry under Sedation
Relative Analgesia
MEET OUR TEAM